Background
Hepatitis, a general term referring to inflammation of the liver, may result from various causes, both infectious (ie, viral, bacterial, fungal, and parasitic organisms) and noninfectious (eg, alcohol, drugs, autoimmune diseases, and metabolic diseases). Hepatitis A is caused by hepatitis A virus (HAV), a positive-sense, single-stranded, nonenveloped RNA virus that belongs to the Picornaviridae family and the Hepatovirus genus. Other viruses known to cause hepatitis include caused by hepatitis A virus (HAV), hepatitis B virus (HBV), hepatitis D virus (HDV), hepatitis E virus (HEV), however, these viruses are they are genetically distinct and unrelated to one another, thus immunity to one does not provide protection against the others. See viral hepatitis, for more information.
After fecal-oral transmission, the virus is then excreted into the bile. Its concentration is highest in the stool, especially during the 2 weeks preceding the onset of jaundice. This correlates with the period of peak infectivity. Children and adults can be assumed to be noninfectious 1 week after the appearance of jaundice. In most cases, HAV infection is self-limited, and many cases are asymptomatic. Except in the setting of fulminant hepatitis, which is uncommon, sequelae are rare. Relapsing HAV infection occurs in approximately 10% of patients 1-4 months after the initial episode and results in full recovery.
Chronic active hepatitis, which can be seen in HBV or HCV infection, does not occur in HAV infection. A chronic carrier state is also not seen with HAV infection.
The relative frequency of HAV as a cause of acute hepatitis has declined in Western societies due to improvements in hygiene, public health policies, and sanitation. Vaccination and passive immunization have also successfully led to reduction among high-risk groups.
Etiology
Common-source outbreaks of hepatitis A from contaminated food or water may occur. [3] HAV is concentrated in filter-feeding shellfish, which may thrive close to sewage outlets, and widespread outbreaks can occur from a single contaminated source, such as uncooked vegetables that are distributed to restaurants or grocery stores. [4]
Childcare centers may be sources of outbreaks from contaminated changing tables. These outbreaks may not be identified until an adult contact has a recognizable HAV infection, because young children are often asymptomatic or have anicteric illnesses.
Vertical transmission of HAV (ie, from mother to neonate) and transmission by means of blood transfusion are extremely rare. Spread of HAV infection from nonhuman primates (ie, chimpanzees, rhesus monkeys) to humans is possible. [5]
Risk factors for the acquisition of hepatitis A include the following:
-
Personal contacts
-
Institutionalization
-
Occupation (eg, daycare)
-
Foreign travel
-
Male homosexuality
-
Illicit parenteral drug use
-
Homelessness
Pathophysiology
HAV is a single-stranded, positive-sense, linear RNA enterovirus of the Picornaviridae family. In humans, viral replication depends on hepatocyte uptake and synthesis, and assembly occurs primarily in the liver cells. Virus acquisition results almost exclusively from ingestion (eg, fecal-oral transmission), although isolated cases of parenteral transmission have been reported.
HAV is an icosahedral nonenveloped virus, measuring approximately 28 nm in diameter (see the image below). Its resilience is demonstrated by its resistance to denaturation by ether, acid (pH 3.0), drying, and temperatures as high as 56°C and as low as -20°C. The hepatitis A virus can remain viable for many years. Boiling water is an effective means of destroying it. Chlorine and iodine are similarly effective.
Various genotypes of HAV exist; however, there appears to be only 1 serotype. Virion proteins 1 and 3 are the primary sites of antibody recognition and subsequent neutralization. No antibody cross-reactivity has been identified with other viruses causing acute hepatitis. Evidence in recent years appears to show that the exosomes play a dual role in the transmission of HAV and HCV, allowing these viruses to evade antibody-mediated immune responses but, paradoxically, can also be detected by plasmacytoid dendritic cells (pDCs) leading to innate immune activation and type I interferon production. [1]
Liu et al performed phylogenetic and recombination analyses on 31 complete HAV genomes from infected humans and simians. They identified 3 intra-genotypic recombination events (I-III), which they believe demonstrate that humans can be co-infected with different HAV subgenotypes. [2]
The first recombination event (I) occurred between the lineage represented by the Japanese isolate AH2 (AB020565, subgenotype IA), and the second event (II) occurred between the lineage represented by the North African isolate MBB (M20273, subgenotype IB). [2] These 2 recombination events resulted in the recombinant Uruguayan isolate HAV5 (EU131373).
The third recombination event (III) occurred between the North African lineage (isolate MBB; M20273, subgenotype IB) and the German lineage (isolate GBM; X75215, subgenotype IA), leading to the Italian isolate FG (X83302). [2]
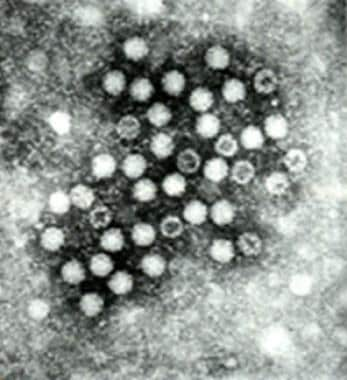
Hepatocyte uptake involves a receptor, identified by Kaplan et al, on the plasma membrane of the cell, and viral replication is believed to occur exclusively in the hepatocytes. The demonstration of HAV in the saliva has raised questions about this exclusivity. After entry into the cell, viral RNA is uncoated, and the host ribosomes bind to form polysomes. Viral proteins are synthesized, and the viral genome is copied by a viral RNA polymerase (see the image below). Assembled virus particles are shed into the biliary tree and excreted in the feces.
Minimal cellular morphologic changes result from hepatocyte infection. The development of an immunologic response to infection is accompanied by a predominantly portal and periportal lymphocytic infiltrate and a varying degree of necrosis.
Many authorities believe that hepatocyte injury is secondary to the host's immunologic response. This hypothesis is supported by the lack of cytotoxic activity in tissue culture and correlations between immunologic response and the manifestations of hepatocyte injury.
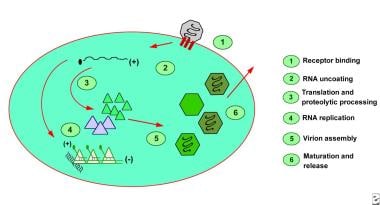
Person-to-person contact is the most common means of transmission and is generally limited to close contacts. Transmission through blood products has been described. The period of greatest shedding of HAV is during the anicteric prodrome (14-21 d) of infection and corresponds to the time when transmission is the highest (see the image below). Recognizing that the active virus is shed after the development of jaundice is important, although the quantity falls rapidly.
Although foodborne outbreaks of acute hepatitis A occur and receive wide-spread media attention, the number of infections is usually minimal. For example, in 2022 and 2023 imported fresh and frozen organic strawberries were linked to 39 confirmed cases of HAV infection in the US and Canada. [3]
Epidemiology
United States statistics
Over the last century, improved sanitation and hygiene measures have resulted in a shift in the age group that carries the burden of hepatitis A. This, in turn, may result in more clinically apparent and severe disease. In 2023, there were an estimated
International statistics
The World Health Organization (WHO) reports that HAV infection is common in developing countries with poor sanitation. Hepatitis A remains a gobal health burden with an estimated 156 million acute cases and 35,500 deaths annually. Overall, 63% of acute hepatitis A cases, and 93% of hepatitis A deaths occurred in low- and lower-middle-income countries. [6]
Age-related demographics
In the United States, prior to targeted vaccination programs, the highest rate of infection occurred in children aged 5-14 years. Since the advent of widespread vaccination, as many as 80% of infections have been in adults.
With increasing age of acquisition, both symptomatic disease and adverse sequelae increase. In Shanghai in 1988, a large shellfish-related epidemic occurred with over 300,000 confirmed cases. Most of those admitted to the hospital were aged 20-40 years. Mortality from fulminant hepatic failure increased with increasing age despite the decreasing prevalence of disease as age increased. The lower incidence of infection in the older population was related to a greater likelihood of immunity rather than to a decrease in exposure. [7]
Sex-related demographics
Globally there is no sexual predilection apparent; In the US men outnumber women 2:1 due to the higher infection rates in high-risk groups (ie, male homosexuals, sewage workers, homeless individuals). [6]
Prognosis
The prognosis is excellent. In most patients, HAV infection is self-limited, and complete recovery occurs. In fact, many cases are asymptomatic. Except in the setting of fulminant hepatitis, sequelae are rare. Fulminant hepatitis due to HAV is uncommon and has a case-fatality rate of 0.4%.
Relapsing HAV infection occurs in approximately 10% of patients 1-4 months after the initial episode and results in full recovery.
Chronic active hepatitis, which can be seen in hepatitis B virus (HBV) or hepatitis C virus (HCV) infection, does not occur in HAV infection. A chronic carrier state is not seen with HAV infection.
Complications
Complications are few. Fulminant hepatitis with massive hepatic necrosis and liver failure due to HAV infection is rare. Cholestatic hepatitis occurs in a small percentage of patients.
Acute renal failure, interstitial nephritis, pancreatitis, red blood cell aplasia, agranulocytosis, bone marrow aplasia, transient heart block, Guillain-Barré syndrome, acute arthritis, Still disease, lupus-like syndrome, and Sjögren syndrome have been reported in association with HAV. These complications are all rare.
Relapsing HAV infection occurs in 3-20% of patients with acute HAV infection and uncommonly takes the form of multiple relapses. After a typical acute course of HAV infection, a remission phase occurs, with partial or complete resolution of clinical and biochemical manifestations. The initial flare usually lasts 3-6 weeks; relapse occurs after a short period (usually < 3 wk) and mimics the initial presentation, although it usually is clinically milder.
Liver transplantation has been performed in patients with this condition when signs of significant decompensation have occurred. Corticosteroid treatment has been shown to improve the clinical course, although the course is generally benign without treatment.
-
Hepatitis A virus as viewed through electron microscopy.
-
Hepatitis A. Time course of infection.
-
Hepatitis A.